


Project Overview
AssistTH was developed as a human-centered telehealth concept to address gaps in remote consultation, patient follow-up, clinical information access, medicine delivery, appointment management, and healthcare accessibility. The project was conducted as a research-driven UX case study involving literature review, contextual inquiry, surveys, interviews, low-fidelity prototyping, high-fidelity prototyping, and usability evaluation.
The broader design challenge was to understand how a telehealth system could support both sides of the consultation: patients who face travel, accessibility, cost, and follow-up barriers, and physicians who need reliable patient information, medical history, vitals, and a trustworthy clinical workflow during remote appointments.
online survey responses used to understand telehealth needs and attitudes
in-person interviews with patients and doctors across multiple hospitals
participants in usability testing across patient-side and doctor-side workflows
My Role and Contributions
I contributed to the full UX research and design process, including problem framing, literature review, contextual inquiry, survey and interview design, user-need analysis, ideation, low-fidelity prototyping, Figma-based high-fidelity prototyping, usability testing, and synthesis of design implications.
My work focused on translating research findings into usable application flows for appointment booking, follow-ups, vitals access, medical-record visibility, medicine ordering, lab-test support, and patient-doctor communication.
Advisor
Dr. Suleman Shahid
Lahore University of Management Sciences
Collaborators
Khuzaima Saeed, Muhammad Hassnain, Mohammad Jahanzeb Raza, and Salman Masood.
Problem Context
Telehealth adoption accelerated during the COVID-19 pandemic, but the usability and trustworthiness of many remote healthcare workflows remained limited [2]. Patients often faced difficulty communicating symptoms, accessing follow-up care, obtaining medicines, and managing appointments. Doctors, in turn, often lacked sufficient access to patient history, vitals, and records during remote consultations.
The problem was therefore not simply to create a video-consultation interface, but to design a more complete telehealth experience that could improve coordination, safety, convenience, and decision support for both patients and physicians.
Design Challenge
How might we design a telehealth application that improves remote consultation quality while supporting patient ease, physician confidence, accessibility, and continuity of care?
Related Work and Domain Review
We reviewed prior work on telehealth, telemonitoring, teleconsultation, telerehabilitation, and digital delivery of care. This helped frame telehealth as a multidimensional healthcare model involving preventive, promotive, and curative care rather than only video-based consultation [1].
Telehealth adoption increased substantially during the COVID-19 pandemic, which made the quality, accessibility, and usability of digital healthcare systems an urgent design concern [2]. We also reviewed patient-facing telehealth experience studies to understand how satisfaction, trust, and perceived usefulness influence remote-care acceptance [3].
Why this mattered for design
The literature showed that telehealth is not only a technical problem. It is also a service-design, trust, workflow, accessibility, and usability problem. This shaped AssistTH as a complete care-support workflow rather than only a video-call interface.
User Research Methodology
We used a mixed-method approach combining surveys, contextual inquiry, and semi-structured interviews. Data were collected from public and private hospitals including Mayo Hospital, Sheikh Zayed Hospital, Services Hospital, Al-Ehsan Hospital, National Hospital, and Akhtar Saeed Hospital.
The participant pool included patients and doctors from different socio-economic, demographic, educational, and professional backgrounds. We also considered groups who often experience additional barriers to healthcare access, including older adults, individuals with disabilities, and patients requiring frequent follow-up appointments.
Interviews were conducted in the language most comfortable for participants, including English, Urdu, and Punjabi. This helped reduce communication barriers and allowed participants to explain healthcare experiences in more natural terms.
User Needs and Research Findings
The research identified distinct but interconnected needs for doctors and patients. Doctors emphasized the importance of understanding appointment intent, viewing symptoms and medical history, checking vitals, and building trust in remote consultations. Patients emphasized travel burden, appointment access, follow-up convenience, medicine ordering, safety, and reduced exposure to crowded hospital environments.
Doctor-Side Challenges
- Lack of clarity about the patient’s appointment objective.
- Difficulty interpreting symptoms without in-person examination.
- Limited access to vitals, history, and medical records.
- Concern about trust and diagnostic confidence in online consultations.
Patient-Side Challenges
- Travel burden for follow-up visits and specialist consultations.
- Difficulty arranging hospital visits, especially for older or disabled patients.
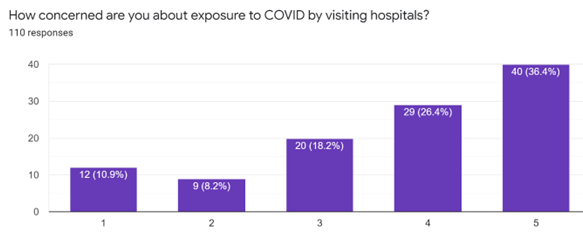
- Concerns about exposure to infectious environments.
- Need for medicine ordering, lab tests, reminders, and follow-up management.
“In Gilgit-Baltistan, army organizes medical camps. The days are announced that an expert of this field will sit on this day, and that is how we get medical checkups once a year. I would personally be willing to use an online health service.”
Doctor-Side Evidence
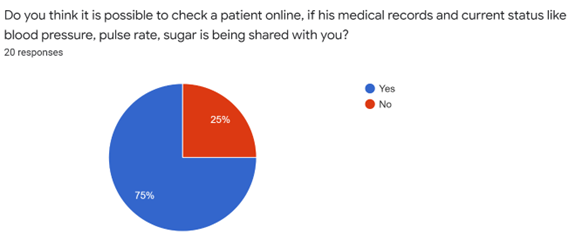
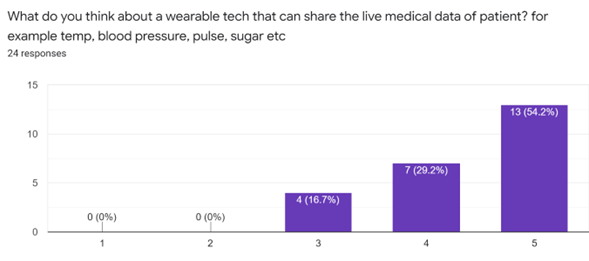
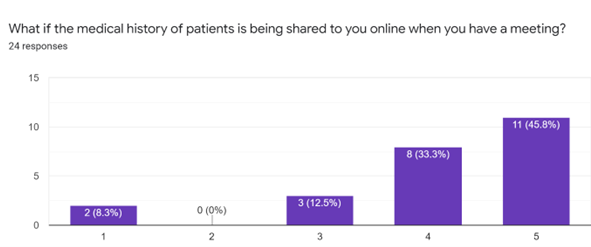
Doctors reported that remote consultations become more acceptable when the system provides structured patient information. In particular, access to vitals and medical records increased confidence in online consultation workflows.
Patient-Side Evidence
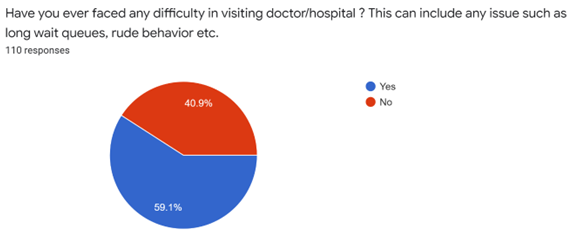
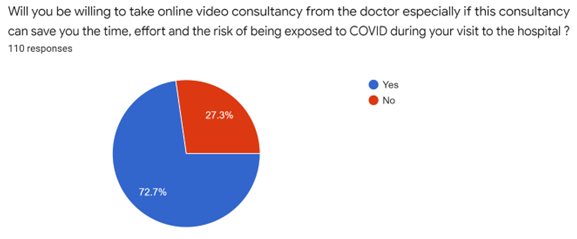
Patient research showed that travel burden, hospital fatigue, exposure concerns, and difficulty managing follow-ups were major reasons for considering telehealth. Many participants were willing to use remote follow-up services if the system was reliable, understandable, and trustworthy.
Design Process
Based on user research, we evaluated seven design alternatives using six criteria: trust, reliability, quality, accessibility, feasibility, and efficiency. The final concept combined the most valued elements from different alternatives into a comprehensive telehealth workflow.
The final design included video consultation, appointment scheduling, pick-up support, medicine delivery, lab-test home collection, vitals monitoring, emergency response, reminders, wallet features, subtitles, assistive support, and access to medical records.
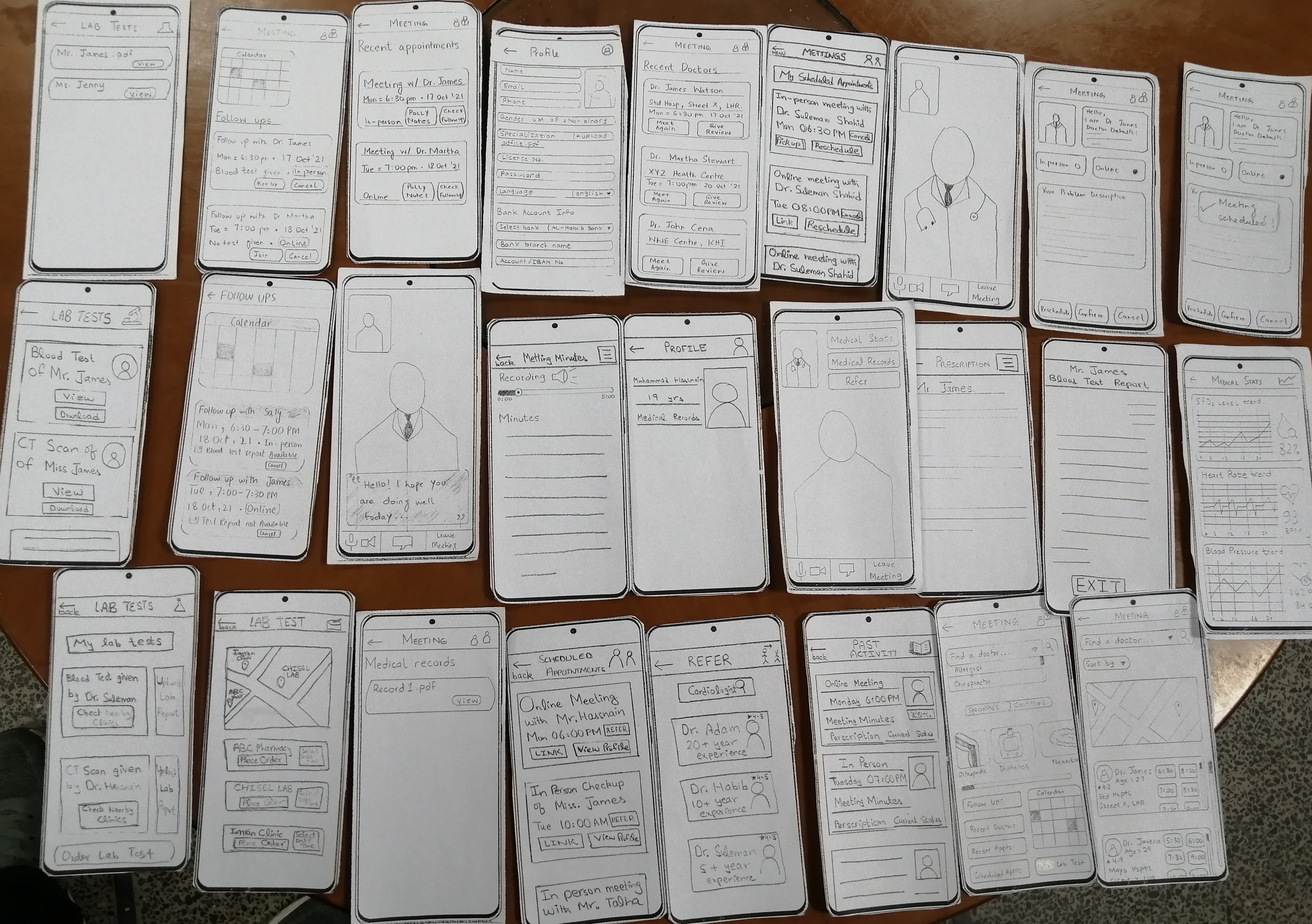
Low-Fidelity Prototyping
We began with low-fidelity sketches and paper prototypes. This allowed rapid iteration and helped test whether users understood the proposed workflows before moving into high-fidelity design.
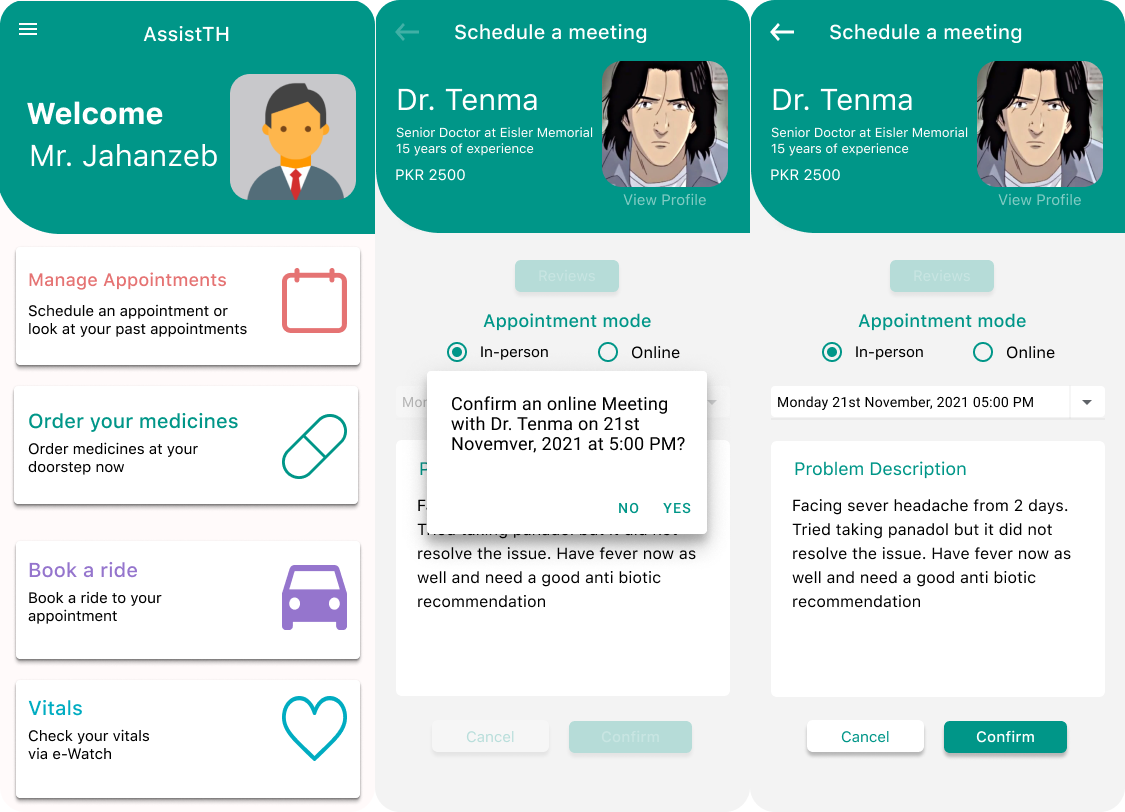
High-Fidelity Prototyping
After pilot feedback on the low-fidelity prototype, we developed high-fidelity screens in Figma. The design emphasized simplicity, learnability, consistency, visibility of system state, accessibility, privacy, and reduced interaction errors.

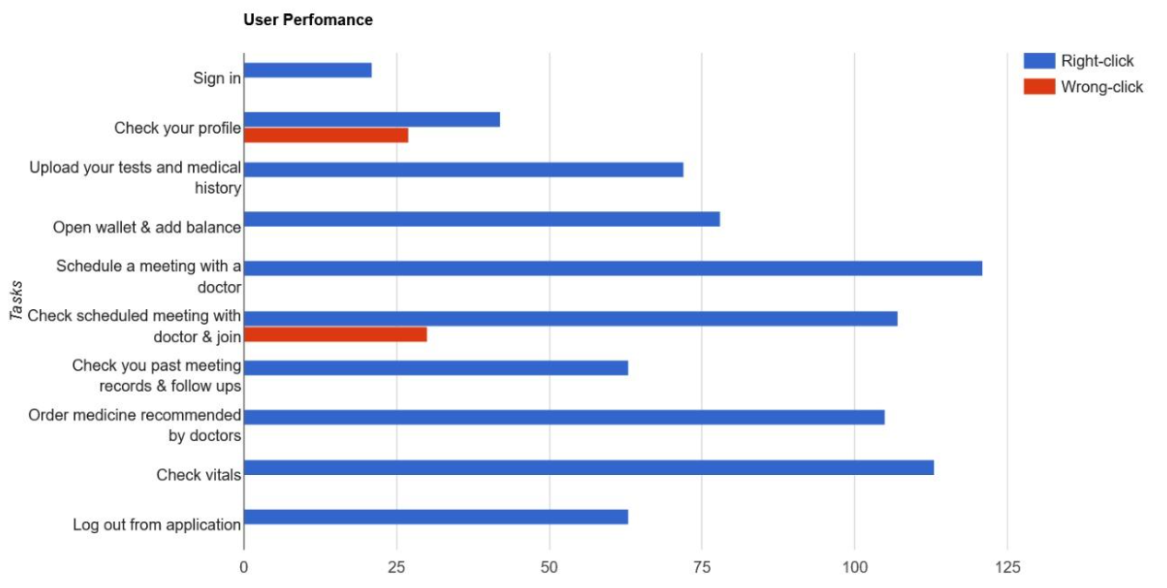
Usability Evaluation
We evaluated both patient-oriented and doctor-oriented workflows. Participants completed scenario-based tasks while we recorded task completion, wrong clicks, completion time, questionnaire responses, and qualitative feedback.
Patient-Side Tasks
- Sign in or log in.
- Schedule a meeting with a doctor.
- Join a scheduled appointment.
- Check past meetings and follow-ups.
- Order medicine from a pharmacy.
- Order lab tests.
- Check vitals and use side-menu functions.
- Log out.
Doctor-Side Tasks
- Sign in or log in.
- Check profile information.
- View scheduled meetings.
- Join appointments and review vitals and records.
- Check past meetings and follow-ups.
- Open wallet and view earnings.
- Log out.
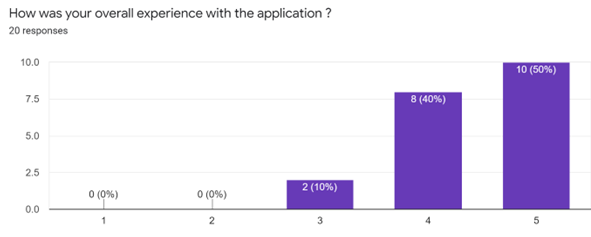
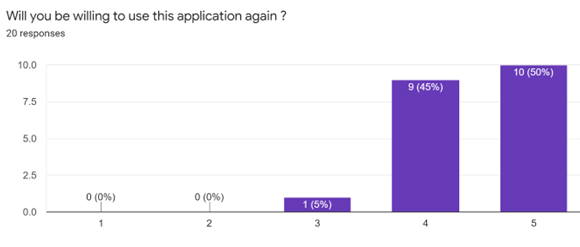
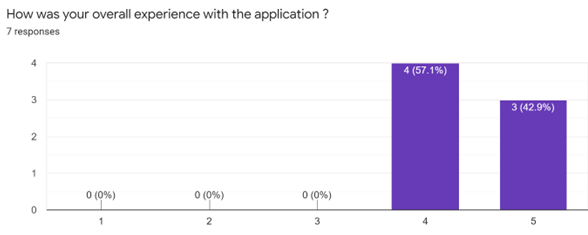
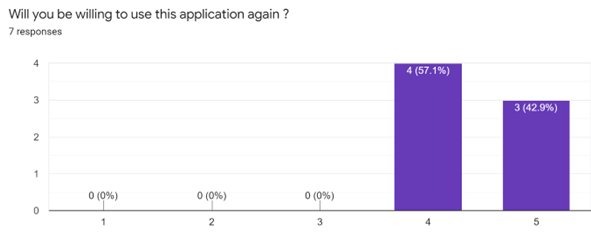
Quantitative Usability Results
Post-test feedback showed positive responses from both patients and doctors. Participants generally found the system understandable and useful, and many were able to complete tasks with few wrong clicks.
Qualitative Usability Insights
Participants responded positively to the interface clarity, workflow organization, and visual design. They appreciated having appointments, medication orders, test results, follow-ups, and vitals in one place.
The design was described as clear and easy to understand. Participants also noted that the application could reduce effort by centralizing multiple healthcare tasks. Some participants, however, identified areas for improvement, including clearer icons, reduced screen complexity, improved visibility of system state, and stronger signals of privacy and legitimacy.
Design Implication
Users valued convenience and centralization, but trust, privacy, clarity, and reduced cognitive load remain essential for telehealth adoption.
Contribution and Impact
AssistTH contributes a user-centered telehealth concept grounded in both patient and doctor needs. The project identifies practical design requirements for remote healthcare, including access to patient vitals, medical records, follow-up management, medicine delivery, appointment scheduling, and accessibility support.
The case study also demonstrates how contextual inquiry, literature review, prototype testing, and usability evaluation can be combined to design a more complete healthcare service experience rather than a narrow video-call interface.
Limitations and Future Work
The study was limited by time, access, and resource constraints. Data collection was affected by hospital access limitations and COVID-19 restrictions. Cultural factors also made it difficult to maintain equal gender balance in all participant groups.
Usability testing was also limited because several participants were recruited within the LUMS environment, which may not fully represent broader patient and healthcare-provider populations. Future work should include larger samples, more diverse patient groups, more healthcare providers, and testing in realistic clinical contexts.
Conclusion
AssistTH shows how a telehealth system can be designed through a rigorous user-centered process. By combining patient needs, physician concerns, healthcare workflow analysis, prototyping, and usability testing, the project proposes a more integrated model for digital healthcare access.
The project also highlights that successful telehealth design depends not only on technology, but also on trust, accessibility, continuity of care, medical information availability, and careful interaction design.
Skills, Tools & Frameworks
References
- M. Ade, N. Doulamis, S. S. Wagle, and M. G. Ullah, “TeleHealth: Healthcare technologies and TeleHealth Emergency (THE) system,” 2011 2nd International Conference on Wireless Communication, Vehicular Technology, Information Theory and Aerospace & Electronic Systems Technology, 2011, pp. 1-4. doi: 10.1109/WIRELESSVITAE.2011.5940870.
- L. M. Koonin et al., “Trends in the use of telehealth during the emergence of the COVID-19 pandemic, United States, January-March 2020,” MMWR Morbidity and Mortality Weekly Report, vol. 69, pp. 1595-1599, 2020.
- K. Y. Capusan and T. Fenster, “Patient satisfaction with telehealth during the COVID-19 pandemic in a pediatric pulmonary clinic,” Journal of Pediatric Health Care, 2021. doi: 10.1016/j.pedhc.2021.07.014.